
Hypermobility and Ehlers-Danlos Syndrome Symptoms are Explained by Abnormal Sympathetic Responses to Head-Up Postural Change
Nicholas L. DePace, MD, FACC; Stephen Soloway, MD, FACP, FACR; Joe Colombo, PhD, DNM, DHS
SUMMARY
Background
Ehlers-Danlos Syndrome, hypermobility type (EDSh), is a heritable connective tissue disorder characterized by joint hypermobility, frequent subluxations, and “leaky” collagen. Beyond musculoskeletal manifestations, EDSh patients frequently present with autonomic dysfunction (AD), which drives many of their systemic symptoms including chronic pain, inflammation, fatigue, orthostatic intolerance, palpitations, gastrointestinal dysmotility, cognitive impairment, and migraine.
A key autonomic abnormality in this population is Sympathetic Withdrawal (SW), an abnormal alpha-adrenergic failure to mount a sympathetic response upon standing. SW is linked to orthostatic dysfunction (OD) and contributes to reduced cerebral perfusion, leading to debilitating symptoms.
Methods
From November 2018 to May 2020, 569 EDSh patients (94.2% female, mean age 30.4 years) were referred to a cardiovascular/autonomic clinic in the northeastern USA. Diagnosis was confirmed via rheumatology and standardized criteria (Beighton scoring and Ehlers-Danlos Society checklist).
All patients underwent comprehensive assessment including vestibular testing, mast cell labs, small fiber neuropathy testing, cardiology work-up, and serial P&S monitoring (Physio PS, Atlanta, GA), providing direct measures of:
LFa = sympathetic activity
RFa = parasympathetic activity
SB = sympathovagal balance
SW was defined as a paradoxical sympathetic decrease upon postural change. Treatment included r-Alpha Lipoic Acid (rALA) and titrated low-dose vasoactive medications, with long-term rALA for maintenance.
Results
Sympathetic Withdrawal (SW): Detected in 49.4% of the cohort, predominantly younger patients.
Orthostatic Dysfunction: 104 patients exhibited orthostatic hypotension. P&S monitoring identified OH risk more reliably than HRV alone (p = 0.009).
Morbidity/Mortality: Only 14.4% demonstrated advanced AD. No patients <65 years showed late-stage autonomic neuropathy. EDSh does not appear to increase natural mortality risk, but does impair productivity and quality of life.
Symptom profile: Common complaints included diffuse musculoskeletal pain, palpitations, dizziness/fainting, fatigue, brain fog, sleep disturbance, and hypersensitivity to light/sound—consistent with AD manifestations.
Therapeutic response: Relieving SW improved symptoms in >85% of affected patients, restoring quality of life and productivity. Residual cases involved overlapping dysautonomias or comorbidities.
Conclusion
Sympathetic Withdrawal is a highly prevalent but underrecognized autonomic dysfunction in EDSh patients. Standard HRV alone may miss its detection; direct parasympathetic and sympathetic measures are necessary. Treatment with rALA and low-dose vasoactives is effective in restoring autonomic balance and significantly improving patient outcomes. Although EDSh cannot be cured, addressing SW offers a pathway to meaningful quality-of-life restoration.
Hypermobility and Ehlers-Danlos Syndrome Symptoms are Explained by Abnormal Sympathetic Responses to Head-Up Postural Change
Stephen Soloway, MD, FACP, FACR; Nicholas L. DePace, MD, FACC; Joe Colombo, PhD, DNM, DHS
INTRODUCTION
Hypermobility and Ehlers-Danlos Syndrome (EDSh) often present with a constellation of symptoms that are thought to be associated with the connective tissue disorder, and they are, but not directly. The disordered connective tissue leads to Autonomic Dysfunction (AD). EDSh is a genetic disorder of the collagen produced by the human body (hereditary – autosomal dominant – or less frequently, de-novo). It is characterized by joints being quite flexible and oftentimes subluxing, or popping out. It is not unusual for the patients to have their knees, elbows, ankles, wrists, and even jaw pop out, or their cervical spine hypermobile. Even hyper-flexibility in the lumbar spine may make the patient able to touch the ground with their palms with straight knees quite easily. The flexibility is enabled by long, stretchy (rather than short and stiff) collagen, which also causes “leaky” connective tissue.
The leaky connective tissue leads, or contributes, to AD [1,2]. AD leads or contributes to many of the symptoms of EDSh. These symptoms include: diffuse pain, especially in the shoulders, upper back, inter-scapular area, jaw, and hips; excess and persistent inflammation; shortness of breath and palpitations; lightheadedness perhaps with a history of fainting or near-fainting, and oftentimes having to lie down when trying to stand for periods of time; (extreme) fatigue; sleep and GI difficulties, and they cannot get going in the morning; brain fog or memory and cognitive difficulties; and bright light or sound may disturb them, including triggering headache or migraine.
The pain and inflammation symptoms are examples of contributions from AD. For example, the “leaky” connective tissue permits foreign substances to enter the body that normally would not. This causes the immune system to be persistently hyper-active, which causes the Parasympathetic branch to become persistently hyper-active which in turn causes hyper-reactive Sympathetic responses, amplifying the pain response and exacerbating the inflammatory response [3]. Headache, Migraine, and GI difficulties may result directly or indirectly from ADs. The remaining symptoms listed are considered direct results of ADs. The main AD that underlies these symptoms is known as Sympathetic Withdrawal (SW, an alpha-adrenergic dysfunction associated with the range of Orthostatic Dysfunctions, OD) [4]. Here, we describe SW and document its effect within a large clinical cohort of EDSh patients.
METHODS
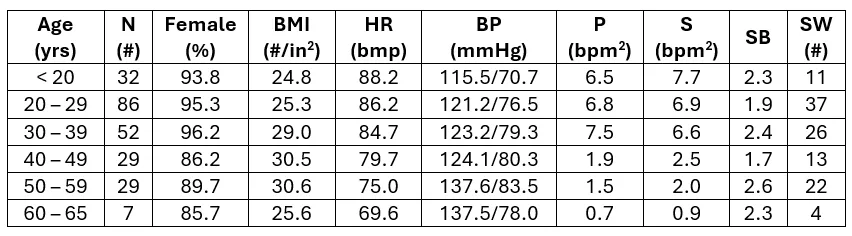
From a single, suburban, cardiovascular and AD clinic in the northeastern United States of America (USA), 569 patients (226 female, 94.2%; average age 30.4yrs, range 13 to 65 y/o; average height 64.5 in; and average weight 158.3#) previously diagnosed by Rheumatology with EDSh were referred from November 2018 through May 2020. This patient cohort included a significant number of patients from across the USA and abroad. Detailed patient histories and physicals were taken as routine, including completing a Beighton Scoring test and the EDSh Diagnostic Checklist from the Ehlers-Danlos Society (www.ehlers-danlos.com). Testing included Vestibular testing; Mast Cell blood work; Small Fiber Neuropathy testing; age- and symptom-specific cardiology testing; and serial P&S Monitoring (Physio PS, Atlanta, GA), which includes HRV measures [5,6]. P&S Monitoring includes LFa as the direct measure of Sympathetic (S) activity, RFa as the direct measure of Parasympathetic (P) activity, and Sympathovagal Balance (SB=S/P, measured at rest as the average of ratios, not the ratio of averages) [4]. These are all quick, in-office tests. All patients had a minimum of two follow-up tests.
SW is an abnormal alpha-adrenergic (Sympathetic) decrease in response to upright postural change (sitting up or standing up). Normally, the alpha-adrenergic response to upright postural change is to increase. The treatment to reverse SW used in this study included the antioxidant r-Alpha-Lipoic Acid (rALA) [3,7] in combination with low-dose oral vasoactive medications [3,8]. Close observation is recommended during the early stages of therapy since the vasoactives tend to raise resting BP while the body acclimates to the restored vasoconstriction. Further, the restored vasoconstriction may also cause additional symptoms (i.e., “goose-bumps” “itchy” scalp, and chest tightness) that may also be distracting. The patient needs to be reassured that these symptoms are indications that the therapy is working, and they normally are relieved naturally in two weeks. To minimize these additional symptoms, and to maximize patient acceptance, the low dose vasoactives are titrated very slowly from even smaller doses. Once SW is relieved, due to the persistent nature of EDSh, a maintenance dose of rALA was required to help maintain normal autonomic function.
Occasionally, SW may be masked by an excessive Parasympathetic response to upright posture. In these cases, both the SW and the PE were treated simultaneously, since these responses are from two different portions of the nervous system [4].
RESULTS
While resting P&S balance (SB, see Table) for the cohort is well within normal limits (SB: 0.4 < SB < 3.0, unitless); preferred SB for younger, < 65 y/o, healthier subjects is 1.0 < SB < 3.0; and preferred SB for older subjects, ≥ 65 y/o, and sicker patients is 0.4 < SB < 1.0; the latter is known to be cardio-protective [9] and protective of bodily systems in general. No patients in the age range of the cohort (< 65 y/o) demonstrate late stage autonomic neuropathy. In other words, EDSh does not affect natural mortality risk. Only 25 patients total (14.4%) demonstrated advanced AD. In other words, EDSh also does not affect natural morbidity risk beyond what is common from the AD directly associated with EDSh. SW occurs in approximately half (49.4%) of this cohort. The majority of patients presenting with SW are younger. This may be in part due to the heavy focus on dysautonomia within the representative practices.
Comparing the change in HRV measures of LF and LF/HF from rest to head-up posture with the change in BP over the same time periods, 104 patients demonstrate a decrease in BP, indicating Orthostatic Hypotension (OH) or pre-clinical OH. Under the same conditions, the change in LF indicates that 151 patients are at risk for OH (19.3% false positive and 48.1% false negative, p = 0.116) and the change in LF/HF indicates that 81 patients are at risk for OH (9.5% false positive and 29.2% false negative, p = 0.067). This is in keeping with the findings of the standards articles, that the LF/HF ratio is better than LF in indicating risk of OH.
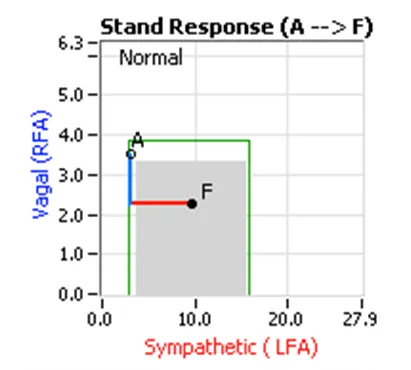
Comparing the change in the P&S measure of Sympathetic activity, LFa, under these same conditions indicates that 120 patients are at risk for OH (6.6% false positive and 3.3% false negative, p = 0.009). A normal P&S stand response is depicted in the Figure (top panel). Normally, the Parasympathetics decrease first to potentiate and minimize the (alpha-)Sympathetic response. Then, the Sympathetics respond positively to cause the vasoconstriction required to defeat gravity and coordinate the Orthostatic response to head-up postural change (e.g., standing).
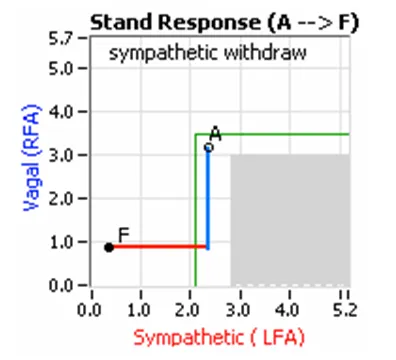
An example of SW is depicted in the Figure (bottom panel), where even though the Parasympathetics decrease as normal, the Sympathetics decrease also. As a result, the Orthostatic response is abnormal, typically resulting in abnormal hemodynamic responses, including Orthostatic Hypotension (OH, SW with a drop in BP upon standing) or Postural Orthostatic Tachycardia Syndrome (POTS, SW with an excessive increase HR upon standing) or Orthostatic Intolerance (OI, SW with a normal hemodynamic response upon standing). Masked SW (if a stand beta-Sympathetic Excess is demonstrated) is demonstrated if a form of OD is indicated. [4,10]
SW was reported in 120 of the 243 (49.4%) patients in this cohort. Relieving SW relieved symptoms in over 85% of this sub-population and helped to restore their quality of life and productivity in society. The remaining EDSh patients in this sub-population had other dysautonomias and confounding disorders that prolonged their therapy.
DISCUSSION
OD is often the first and arguably the most debilitating form of AD [11,12]. The ANS, including its two branches, is a very dynamic system and never actually “rests.” In fact, when the body is at rest, as in sleeping, it may be argued that the P&S systems are most active. This is important because most ADs are not well documented when the patient is at rest. In fact, the primary ADs documented at rest are much later stage dysfunctions [4], such as Diabetic Autonomic Neuropathy or Advanced Autonomic Dysfunction and Cardiovascular Autonomic Neuropathy. These are conditions indicating that patients are already at increased morbidity [11] and mortality [12] risk, respectively. This may be a reason why EDSh symptoms have failed to be associated with AD, because these tend to be younger patients, tested at rest, before most would consider AD. As expected, EDSh seems to affect morbidity and thereby quality of life and productivity, even though common physiologic measures (i.e., HR & BP) are well within normal ranges.
To compound the problem that most ADs are not well documented when the patient is at rest, is the fact that Heart Rate Variability (HRV), a standard measure of autonomic activity, is a mixed measure of P&S responses. Given that the P&S branches work synergistically and attempt to remain in balance, the total responses measured tend to look normal in younger patients.
Standard HRV measures from spectral analysis include Low Frequency (LF) and the ratio of low to high frequency (LF/HF). LF is a mixed measure of P&S activity; however, it is assumed to be primarily a measure of Sympathetic activity. Although, the standards articles [5,6] state that the ratio of LF/HF is found to be a better measure of the change in Sympathetic activity with standing than LF alone. Perhaps the thinking is that HF is assumed to measure Parasympathetic activity, and therefore will yield a more pure measure of Sympathetic activity from the ratio, LF/HF, by dividing out some of the Parasympathetic activity. In fact, HF is a mixed measure of Parasympathetic activity and noise, when the respiratory frequency is high enough; otherwise, it is just noise. [4]
P&S Monitoring enables a direct measure of SW. Some of the symptoms of the typical EDSh patient are: 1) diffuse pain, especially in the shoulders, upper back, and inter-scapular area; 2) shortness of breath and palpitations; 3) inability to stand for long periods of time without lightheadedness or dizziness, often with a history of fainting or near-fainting, and oftentimes needing to lie down when trying to stand for periods of time; 4) extreme tiredness or persistent fatigue (that does not necessarily qualify as chronic fatigue syndrome); 5) sleep difficulties and difficulty getting going in the morning; 6) brain fog or memory and cognitive difficulties; 7) frequent headache or migraine; 8) edema of the legs, ankles, and feet; and 9) sensitivity to bright light or sound. All of these may be explained by poor cerebral perfusion due to OD, caused or contributed to by SW.
The diffuse pain in areas above the heart may be a result of poor perfusion of any structure above the heart. Shortness of breath and palpitations may be a result of poor cardiac perfusion or poor cerebral perfusion leading to the brain releasing adrenaline to stimulate the heart, or both. Of course, lightheadedness is caused by poor cerebral perfusion (including Cranial Nerves), and so dizziness may be due to either or both central vestibular degradation due to poor cerebral perfusion or peripheral vestibular degradation due to poor perfusion above the heart. The inability to stand for long periods of time may be a combination of edema and associated pain in the lower extremities and lightheadedness.
OD is often the first and arguably the most debilitating form of AD [11,12]. The ANS, including its two branches, is a very dynamic system and never actually “rests.” In fact, when the body is at rest, as in sleeping, it may be argued that the P&S systems are most active. This is important because most ADs are not well documented when the patient is at rest. In fact, the primary ADs documented at rest are much later stage dysfunctions [4], such as Diabetic Autonomic Neuropathy or Advanced Autonomic Dysfunction and Cardiovascular Autonomic Neuropathy. These are conditions indicating that patients are already at increased morbidity [11] and mortality [12] risk, respectively. This may be a reason why EDSh symptoms have failed to be associated with AD, because these tend to be younger patients, tested at rest, before most would consider AD. As expected, EDSh seems to affect morbidity and thereby quality of life and productivity, even though common physiologic measures (i.e., HR & BP) are well within normal ranges.
To compound the problem that most ADs are not well documented when the patient is at rest, is the fact that Heart Rate Variability (HRV), a standard measure of autonomic activity, is a mixed measure of P&S responses. Given that the P&S branches work synergistically and attempt to remain in balance, the total responses measured tend to look normal in younger patients.
Standard HRV measures from spectral analysis include Low Frequency (LF) and the ratio of low to high frequency (LF/HF). LF is a mixed measure of P&S activity; however, it is assumed to be primarily a measure of Sympathetic activity. Although, the standards articles [5,6] state that the ratio of LF/HF is found to be a better measure of the change in Sympathetic activity with standing than LF alone. Perhaps the thinking is that HF is assumed to measure Parasympathetic activity, and therefore will yield a more pure measure of Sympathetic activity from the ratio, LF/HF, by dividing out some of the Parasympathetic activity. In fact, HF is a mixed measure of Parasympathetic activity and noise, when the respiratory frequency is high enough; otherwise, it is just noise. [4]
P&S Monitoring enables a direct measure of SW. Some of the symptoms of the typical EDSh patient are: 1) diffuse pain, especially in the shoulders, upper back, and inter-scapular area; 2) shortness of breath and palpitations; 3) inability to stand for long periods of time without lightheadedness or dizziness, often with a history of fainting or near-fainting, and oftentimes needing to lie down when trying to stand for periods of time; 4) extreme tiredness or persistent fatigue (that does not necessarily qualify as chronic fatigue syndrome); 5) sleep difficulties and difficulty getting going in the morning; 6) brain fog or memory and cognitive difficulties; 7) frequent headache or migraine; 8) edema of the legs, ankles, and feet; and 9) sensitivity to bright light or sound. All of these may be explained by poor cerebral perfusion due to OD, caused or contributed to by SW.
The diffuse pain in areas above the heart may be a result of poor perfusion of any structure above the heart. Shortness of breath and palpitations may be a result of poor cardiac perfusion or poor cerebral perfusion leading to the brain releasing adrenaline to stimulate the heart, or both. Of course, lightheadedness is caused by poor cerebral perfusion (including Cranial Nerves), and so dizziness may be due to either or both central vestibular degradation due to poor cerebral perfusion or peripheral vestibular degradation due to poor perfusion above the heart. The inability to stand for long periods of time may be a combination of edema and associated pain in the lower extremities and lightheadedness.
OD is often the first and arguably the most debilitating form of AD [11,12]. The ANS, including its two branches, is a very dynamic system and never actually “rests.” In fact, when the body is at rest, as in sleeping, it may be argued that the P&S systems are most active. This is important because most ADs are not well documented when the patient is at rest. In fact, the primary ADs documented at rest are much later stage dysfunctions [4], such as Diabetic Autonomic Neuropathy or Advanced Autonomic Dysfunction and Cardiovascular Autonomic Neuropathy. These are conditions indicating that patients are already at increased morbidity [11] and mortality [12] risk, respectively. This may be a reason why EDSh symptoms have failed to be associated with AD, because these tend to be younger patients, tested at rest, before most would consider AD. As expected, EDSh seems to affect morbidity and thereby quality of life and productivity, even though common physiologic measures (i.e., HR & BP) are well within normal ranges.
To compound the problem that most ADs are not well documented when the patient is at rest, is the fact that Heart Rate Variability (HRV), a standard measure of autonomic activity, is a mixed measure of P&S responses. Given that the P&S branches work synergistically and attempt to remain in balance, the total responses measured tend to look normal in younger patients.
Standard HRV measures from spectral analysis include Low Frequency (LF) and the ratio of low to high frequency (LF/HF). LF is a mixed measure of P&S activity; however, it is assumed to be primarily a measure of Sympathetic activity. Although, the standards articles [5,6] state that the ratio of LF/HF is found to be a better measure of the change in Sympathetic activity with standing than LF alone. Perhaps the thinking is that HF is assumed to measure Parasympathetic activity, and therefore will yield a more pure measure of Sympathetic activity from the ratio, LF/HF, by dividing out some of the Parasympathetic activity. In fact, HF is a mixed measure of Parasympathetic activity and noise, when the respiratory frequency is high enough; otherwise, it is just noise. [4]
P&S Monitoring enables a direct measure of SW. Some of the symptoms of the typical EDSh patient are: 1) diffuse pain, especially in the shoulders, upper back, and inter-scapular area; 2) shortness of breath and palpitations; 3) inability to stand for long periods of time without lightheadedness or dizziness, often with a history of fainting or near-fainting, and oftentimes needing to lie down when trying to stand for periods of time; 4) extreme tiredness or persistent fatigue (that does not necessarily qualify as chronic fatigue syndrome); 5) sleep difficulties and difficulty getting going in the morning; 6) brain fog or memory and cognitive difficulties; 7) frequent headache or migraine; 8) edema of the legs, ankles, and feet; and 9) sensitivity to bright light or sound. All of these may be explained by poor cerebral perfusion due to OD, caused or contributed to by SW.
The diffuse pain in areas above the heart may be a result of poor perfusion of any structure above the heart. Shortness of breath and palpitations may be a result of poor cardiac perfusion or poor cerebral perfusion leading to the brain releasing adrenaline to stimulate the heart, or both. Of course, lightheadedness is caused by poor cerebral perfusion (including Cranial Nerves), and so dizziness may be due to either or both central vestibular degradation due to poor cerebral perfusion or peripheral vestibular degradation due to poor perfusion above the heart. The inability to stand for long periods of time may be a combination of edema and associated pain in the lower extremities and lightheadedness.
OD is often the first and arguably the most debilitating form of AD [11,12]. The ANS, including its two branches, is a very dynamic system and never actually “rests.” In fact, when the body is at rest, as in sleeping, it may be argued that the P&S systems are most active. This is important because most ADs are not well documented when the patient is at rest. In fact, the primary ADs documented at rest are much later stage dysfunctions [4], such as Diabetic Autonomic Neuropathy or Advanced Autonomic Dysfunction and Cardiovascular Autonomic Neuropathy. These are conditions indicating that patients are already at increased morbidity [11] and mortality [12] risk, respectively. This may be a reason why EDSh symptoms have failed to be associated with AD, because these tend to be younger patients, tested at rest, before most would consider AD. As expected, EDSh seems to affect morbidity and thereby quality of life and productivity, even though common physiologic measures (i.e., HR & BP) are well within normal ranges.
To compound the problem that most ADs are not well documented when the patient is at rest, is the fact that Heart Rate Variability (HRV), a standard measure of autonomic activity, is a mixed measure of P&S responses. Given that the P&S branches work synergistically and attempt to remain in balance, the total responses measured tend to look normal in younger patients.
Standard HRV measures from spectral analysis include Low Frequency (LF) and the ratio of low to high frequency (LF/HF). LF is a mixed measure of P&S activity; however, it is assumed to be primarily a measure of Sympathetic activity. Although, the standards articles [5,6] state that the ratio of LF/HF is found to be a better measure of the change in Sympathetic activity with standing than LF alone. Perhaps the thinking is that HF is assumed to measure Parasympathetic activity, and therefore will yield a more pure measure of Sympathetic activity from the ratio, LF/HF, by dividing out some of the Parasympathetic activity. In fact, HF is a mixed measure of Parasympathetic activity and noise, when the respiratory frequency is high enough; otherwise, it is just noise. [4]
P&S Monitoring enables a direct measure of SW. Some of the symptoms of the typical EDSh patient are: 1) diffuse pain, especially in the shoulders, upper back, and inter-scapular area; 2) shortness of breath and palpitations; 3) inability to stand for long periods of time without lightheadedness or dizziness, often with a history of fainting or near-fainting, and oftentimes needing to lie down when trying to stand for periods of time; 4) extreme tiredness or persistent fatigue (that does not necessarily qualify as chronic fatigue syndrome); 5) sleep difficulties and difficulty getting going in the morning; 6) brain fog or memory and cognitive difficulties; 7) frequent headache or migraine; 8) edema of the legs, ankles, and feet; and 9) sensitivity to bright light or sound. All of these may be explained by poor cerebral perfusion due to OD, caused or contributed to by SW.
The diffuse pain in areas above the heart may be a result of poor perfusion of any structure above the heart. Shortness of breath and palpitations may be a result of poor cardiac perfusion or poor cerebral perfusion leading to the brain releasing adrenaline to stimulate the heart, or both. Of course, lightheadedness is caused by poor cerebral perfusion (including Cranial Nerves), and so dizziness may be due to either or both central vestibular degradation due to poor cerebral perfusion or peripheral vestibular degradation due to poor perfusion above the heart. The inability to stand for long periods of time may be a combination of edema and associated pain in the lower extremities and lightheadedness.
OD is often the first and arguably the most debilitating form of AD [11,12]. The ANS, including its two branches, is a very dynamic system and never actually “rests.” In fact, when the body is at rest, as in sleeping, it may be argued that the P&S systems are most active. This is important because most ADs are not well documented when the patient is at rest. In fact, the primary ADs documented at rest are much later stage dysfunctions [4], such as Diabetic Autonomic Neuropathy or Advanced Autonomic Dysfunction and Cardiovascular Autonomic Neuropathy. These are conditions indicating that patients are already at increased morbidity [11] and mortality [12] risk, respectively. This may be a reason why EDSh symptoms have failed to be associated with AD, because these tend to be younger patients, tested at rest, before most would consider AD. As expected, EDSh seems to affect morbidity and thereby quality of life and productivity, even though common physiologic measures (i.e., HR & BP) are well within normal ranges.
To compound the problem that most ADs are not well documented when the patient is at rest, is the fact that Heart Rate Variability (HRV), a standard measure of autonomic activity, is a mixed measure of P&S responses. Given that the P&S branches work synergistically and attempt to remain in balance, the total responses measured tend to look normal in younger patients.
Standard HRV measures from spectral analysis include Low Frequency (LF) and the ratio of low to high frequency (LF/HF). LF is a mixed measure of P&S activity; however, it is assumed to be primarily a measure of Sympathetic activity. Although, the standards articles [5,6] state that the ratio of LF/HF is found to be a better measure of the change in Sympathetic activity with standing than LF alone. Perhaps the thinking is that HF is assumed to measure Parasympathetic activity, and therefore will yield a more pure measure of Sympathetic activity from the ratio, LF/HF, by dividing out some of the Parasympathetic activity. In fact, HF is a mixed measure of Parasympathetic activity and noise, when the respiratory frequency is high enough; otherwise, it is just noise. [4]
P&S Monitoring enables a direct measure of SW. Some of the symptoms of the typical EDSh patient are: 1) diffuse pain, especially in the shoulders, upper back, and inter-scapular area; 2) shortness of breath and palpitations; 3) inability to stand for long periods of time without lightheadedness or dizziness, often with a history of fainting or near-fainting, and oftentimes needing to lie down when trying to stand for periods of time; 4) extreme tiredness or persistent fatigue (that does not necessarily qualify as chronic fatigue syndrome); 5) sleep difficulties and difficulty getting going in the morning; 6) brain fog or memory and cognitive difficulties; 7) frequent headache or migraine; 8) edema of the legs, ankles, and feet; and 9) sensitivity to bright light or sound. All of these may be explained by poor cerebral perfusion due to OD, caused or contributed to by SW.
The diffuse pain in areas above the heart may be a result of poor perfusion of any structure above the heart. Shortness of breath and palpitations may be a result of poor cardiac perfusion or poor cerebral perfusion leading to the brain releasing adrenaline to stimulate the heart, or both. Of course, lightheadedness is caused by poor cerebral perfusion (including Cranial Nerves), and so dizziness may be due to either or both central vestibular degradation due to poor cerebral perfusion or peripheral vestibular degradation due to poor perfusion above the heart. The inability to stand for long periods of time may be a combination of edema and associated pain in the lower extremities and lightheadedness.
OD is often the first and arguably the most debilitating form of AD [11,12]. The ANS, including its two branches, is a very dynamic system and never actually “rests.” In fact, when the body is at rest, as in sleeping, it may be argued that the P&S systems are most active. This is important because most ADs are not well documented when the patient is at rest. In fact, the primary ADs documented at rest are much later stage dysfunctions [4], such as Diabetic Autonomic Neuropathy or Advanced Autonomic Dysfunction and Cardiovascular Autonomic Neuropathy. These are conditions indicating that patients are already at increased morbidity [11] and mortality [12] risk, respectively. This may be a reason why EDSh symptoms have failed to be associated with AD, because these tend to be younger patients, tested at rest, before most would consider AD. As expected, EDSh seems to affect morbidity and thereby quality of life and productivity, even though common physiologic measures (i.e., HR & BP) are well within normal ranges.
To compound the problem that most ADs are not well documented when the patient is at rest, is the fact that Heart Rate Variability (HRV), a standard measure of autonomic activity, is a mixed measure of P&S responses. Given that the P&S branches work synergistically and attempt to remain in balance, the total responses measured tend to look normal in younger patients.
Standard HRV measures from spectral analysis include Low Frequency (LF) and the ratio of low to high frequency (LF/HF). LF is a mixed measure of P&S activity; however, it is assumed to be primarily a measure of Sympathetic activity. Although, the standards articles [5,6] state that the ratio of LF/HF is found to be a better measure of the change in Sympathetic activity with standing than LF alone. Perhaps the thinking is that HF is assumed to measure Parasympathetic activity, and therefore will yield a more pure measure of Sympathetic activity from the ratio, LF/HF, by dividing out some of the Parasympathetic activity. In fact, HF is a mixed measure of Parasympathetic activity and noise, when the respiratory frequency is high enough; otherwise, it is just noise. [4]
P&S Monitoring enables a direct measure of SW. Some of the symptoms of the typical EDSh patient are: 1) diffuse pain, especially in the shoulders, upper back, and inter-scapular area; 2) shortness of breath and palpitations; 3) inability to stand for long periods of time without lightheadedness or dizziness, often with a history of fainting or near-fainting, and oftentimes needing to lie down when trying to stand for periods of time; 4) extreme tiredness or persistent fatigue (that does not necessarily qualify as chronic fatigue syndrome); 5) sleep difficulties and difficulty getting going in the morning; 6) brain fog or memory and cognitive difficulties; 7) frequent headache or migraine; 8) edema of the legs, ankles, and feet; and 9) sensitivity to bright light or sound. All of these may be explained by poor cerebral perfusion due to OD, caused or contributed to by SW.
The diffuse pain in areas above the heart may be a result of poor perfusion of any structure above the heart. Shortness of breath and palpitations may be a result of poor cardiac perfusion or poor cerebral perfusion leading to the brain releasing adrenaline to stimulate the heart, or both. Of course, lightheadedness is caused by poor cerebral perfusion (including Cranial Nerves), and so dizziness may be due to either or both central vestibular degradation due to poor cerebral perfusion or peripheral vestibular degradation due to poor perfusion above the heart. The inability to stand for long periods of time may be a combination of edema and associated pain in the lower extremities and lightheadedness.
OD is often the first and arguably the most debilitating form of AD [11,12]. The ANS, including its two branches, is a very dynamic system and never actually “rests.” In fact, when the body is at rest, as in sleeping, it may be argued that the P&S systems are most active. This is important because most ADs are not well documented when the patient is at rest. In fact, the primary ADs documented at rest are much later stage dysfunctions [4], such as Diabetic Autonomic Neuropathy or Advanced Autonomic Dysfunction and Cardiovascular Autonomic Neuropathy. These are conditions indicating that patients are already at increased morbidity [11] and mortality [12] risk, respectively. This may be a reason why EDSh symptoms have failed to be associated with AD, because these tend to be younger patients, tested at rest, before most would consider AD. As expected, EDSh seems to affect morbidity and thereby quality of life and productivity, even though common physiologic measures (i.e., HR & BP) are well within normal ranges.
To compound the problem that most ADs are not well documented when the patient is at rest, is the fact that Heart Rate Variability (HRV), a standard measure of autonomic activity, is a mixed measure of P&S responses. Given that the P&S branches work synergistically and attempt to remain in balance, the total responses measured tend to look normal in younger patients.
Standard HRV measures from spectral analysis include Low Frequency (LF) and the ratio of low to high frequency (LF/HF). LF is a mixed measure of P&S activity; however, it is assumed to be primarily a measure of Sympathetic activity. Although, the standards articles [5,6] state that the ratio of LF/HF is found to be a better measure of the change in Sympathetic activity with standing than LF alone. Perhaps the thinking is that HF is assumed to measure Parasympathetic activity, and therefore will yield a more pure measure of Sympathetic activity from the ratio, LF/HF, by dividing out some of the Parasympathetic activity. In fact, HF is a mixed measure of Parasympathetic activity and noise, when the respiratory frequency is high enough; otherwise, it is just noise. [4]
P&S Monitoring enables a direct measure of SW. Some of the symptoms of the typical EDSh patient are: 1) diffuse pain, especially in the shoulders, upper back, and inter-scapular area; 2) shortness of breath and palpitations; 3) inability to stand for long periods of time without lightheadedness or dizziness, often with a history of fainting or near-fainting, and oftentimes needing to lie down when trying to stand for periods of time; 4) extreme tiredness or persistent fatigue (that does not necessarily qualify as chronic fatigue syndrome); 5) sleep difficulties and difficulty getting going in the morning; 6) brain fog or memory and cognitive difficulties; 7) frequent headache or migraine; 8) edema of the legs, ankles, and feet; and 9) sensitivity to bright light or sound. All of these may be explained by poor cerebral perfusion due to OD, caused or contributed to by SW.
The diffuse pain in areas above the heart may be a result of poor perfusion of any structure above the heart. Shortness of breath and palpitations may be a result of poor cardiac perfusion or poor cerebral perfusion leading to the brain releasing adrenaline to stimulate the heart, or both. Of course, lightheadedness is caused by poor cerebral perfusion (including Cranial Nerves), and so dizziness may be due to either or both central vestibular degradation due to poor cerebral perfusion or peripheral vestibular degradation due to poor perfusion above the heart. The inability to stand for long periods of time may be a combination of edema and associated pain in the lower extremities and lightheadedness.
The extreme tiredness or fatigue symptoms, which mimic depression-like symptoms is a direct result of poor cerebral perfusion. In fact, many patients also report bouts of anxiety-like symptoms with the feelings of fatigue and depression. This may be explained by the “adrenaline storms” [13]. The sleep difficulties may be a result of abnormal changes in cerebral perfusion due to SW. For example, while upright (e.g., sitting or standing all day) and due to SW, the brain is only marginally perfused and marginally functional (causing among the others the fatigue). As soon as a supine position is assumed, cerebral perfusion is restored (like falling down after fainting). Now the brain is fully perfused and fully functional. In fact, many patients report being more alert during this time (immediately after lying down in bed) than they were during the day. In effect, the patient’s day and night have been reversed. This leads to difficulty falling asleep, waking frequently during the night (more than twice even to go to the bathroom; the brain is still alert and active), or both. Ultimately, the poor sleep leads to the difficulty getting going in the morning, and compounds the fatigue (and any depression). [14]
Of course, brain fog or memory and cognitive difficulties are a direct result of poor cerebral perfusion, as well as some types of headaches and migraines, and these may also involve sensitivity to bright light or sound. Also, edema of the lower extremities is an obvious result of OH due to SW. Relieving SW helps to relieve the OD, poor cardiac perfusion, and poor cerebral perfusion symptoms associated with SW, in the majority of the cases. [14]
CONCLUSIONS
SW is a largely unrecognized AD that is best measured by independent, simultaneous measures of the ANS. SW is relatively easy to treat, once documented, requiring low dose pharmaceuticals and a natural antioxidant. SW in EDSh patients is often debilitating and simply treating the symptoms often exacerbates the case. Therapy durations are not short, lasting at least 9 months and perhaps up to 24 months depending on the duration and severity of the disorder. More research is needed to find a cure for EDSh directly, but for the time being, a means of restoring quality of life and productivity in these patients is possible.
REFERENCES
1. DePace NL, Acosta CR, DePace Jr. NL, Kaczmarski K, Goldis M, Colombo J. Hypermobility and Ehlers-Danlos Syndrome and the Parasympathetic and Sympathetic Nervous Systems. J Individ Med Ther. 2022, 1(1).
2. DePace NL, Santos, L; Munoz, R; Acosta CR, DePace Jr. NL, Kaczmarski K, Ahmad, G; Verma, A; Goldis M, Colombo J. Abnormal Parasympathetic Responses to Stress Exacerbate Hypermobility and Ehlers-Danlos Syndrome Symptoms. Submitted, JOIMT; 2022.
3. DePace NL, Colombo J. Clinical Autonomic and Mitochondrial Disorders: Diagnosis, Prevention and Treatment for Mind-Body Wellness. Springer Nature Switzerland, AG. 2019.
4. Colombo J, Arora RR, DePace NL, Vinik AI. Clinical Autonomic Dysfunction: Measurement, Indications, Therapies, and Outcomes. Springer Science + Business Media, New York, NY, 2014.
5. Malik, M. The Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability, standards of measurement, physiological interpretation, and clinical use. Circulation. 1996; 93:1043-1065.
6. Malik, M. and the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability, standards of measurement, physiological interpretation, and clinical use. European Heart Journal. 1996, 17: 354-381.
7. Murray GL, Colombo J. (r)Alpha Lipoic Acid Is a Safe, Effective Pharmacologic Therapy of Chronic Orthostatic Hypotension Associated with Low Sympathetic Tone. Int J Angiol. 2019 Sep;28(3):188-193. doi: 10.1055/s-0038-1676957. Epub 2019 Feb 22.
8. DePace NL, Vinik AI, Acosta C, Santos L, Murray GL, and Colombo J. Oral vasoactive medications: A review of midodrine, droxidopa and pseudoephedrine. J Individ Med Ther. 2022, 1(1).
9. Umetani K, Singer DH, McCraty R, and Atkinson M. Twenty-four hour time domain heart rate variability and heart rate: Relations to age and gender over nine decades. JACC. 1998; 31(3), 593 – 601.
10. Arora RR, Bulgarelli RJ, Ghosh-Dastidar S, Colombo J. Autonomic Mechanisms and Therapeutic Implications of Postural Diabetic Cardiovascular Abnormalities. J Diabetes Science and Technology. 2008; 2(4): 568-71.
11. Vinik AI, Maser RE, Nakave AA. Diabetic cardiovascular autonomic nerve dysfunction. US Endocrine Disease. 2007; Dec: 2-9.
12. Vinik A, Ziegler D. Diabetic cardiovascular autonomic neuropathy. Circulation. 2007; 115: 387-397.
13. Colombo J, Murray GL, Pinales JM, Acosta C, Lill R, Friedman, MJ, Parker DJ, and DePace NL. Parasympathetic and sympathetic nervous system monitoring and anxiety-like symptoms: Improved differentiation and improved outcomes. Cardio Open. 2020; 5(1): 19-25. doi: 10.33140/COA.05.01.04
14. DePace NL, Acosta CR, DePace Jr. NL, Kaczmarski K, Goldis M, Santos, L; Munoz, R; Ahmad, G; Verma, A; Colombo J. Hypermobility and Ehlers-Danlos Syndrome Symptoms are Explained by Abnormal Sympathetic Responses to Head-Up Postural Change. J Individ Med Ther. 2022, 1(1).
This syndrome affects just under 200,000 people each year.
People with Ehlers-Danlos Syndrome (EDS) often experience issues with their autonomic nervous system, which controls automatic body functions like heart rate and digestion.
This condition, called dysautonomia, happens when there is an imbalance between two parts of the nervous system: the Parasympathetic (which helps the body relax) and the Sympathetic (which helps the body respond to stress).
While scientists are still exploring what causes EDS, research shows that the nervous system dysfunction linked to the disorder can be identified, diagnosed, and treated. This research is just the beginning...
More studies with larger groups of patients from different backgrounds are needed to better understand and manage EDS as awareness continues to grow.
A defining feature of EDS is autonomic dysfunction,
ALL FORMS OF DYSAUTONOMIA ARE TREATABLE & CURABLE!
Autonomic dysfunction, also known as dysautonomia. Dysautonomia is generally caused by an imbalance between the two branches of the Autonomic Nervous System: the Parasympathetic (rest & digest) and the Sympathetic (fight or flight) nervous systems.
This may help explain the delayed onset of symptoms. During childhood and adolescence, the autonomic nervous system (ANS) is highly active in supporting development, which may mask dysautonomia symptoms.
However, as development slows in the late teens or early twenties, dysautonomia symptoms become more apparent, often resulting in persistent autonomic nervous system overactivity.
What to Know About Identifying EDS
Several key characteristics have been identified:
1) It affects females significantly more than males;
2) In childhood, the increased flexibility may seem beneficial due to a lack of severe symptoms; and
3) Symptoms often emerge in late adolescence or early adulthood, causing previously active individuals to experience a decline in health and quality of life.

Patients with EDS often experience widespread pain, particularly in the shoulders, upper back, between the shoulder blades, jaw, and hips. Many report joint hypermobility, with frequent subluxations (partial dislocations) or joints popping out of place, affecting the knees, elbows, ankles, wrists, jaw, and even the cervical spine.
Hyper-flexibility in the lumbar spine may also allow some individuals to touch the ground with their palms while keeping their knees straight.
In addition to musculoskeletal symptoms, patients commonly report shortness of breath, palpitations, dizziness, and fainting or near-fainting episodes, particularly when standing for extended periods.
Fatigue is another major concern, with patients struggling to wake up in the morning, experiencing persistent exhaustion, and having difficulty with concentration, memory, and cognitive function (commonly called "brain fog").
Sensitivity to bright lights or loud sounds is also frequently noted.
These symptoms—aside from joint issues—are linked to dysautonomia, which can also contribute to amplified pain and Fibromyalgia-like symptoms.

Many Patients Recall Being Athletic In Childhood
Often excelling in dance or gymnastics due to their flexibility. They may describe themselves as "double-jointed." A family history of similar symptoms can be a key diagnostic clue in determining whether a patient has Ehlers-Danlos Syndrome.
Physical signs include soft, hyper-extensible (overly stretchy) skin, particularly if the skin on the non-dominant forearm stretches more than 2 cm. The skin may also feel velvety, and patients may have stretch marks (striae) on their back, thighs, breasts, or abdomen.
Additionally, there may be a history of recurrent abdominal or inguinal hernias. Some patients report childhood pelvic floor abnormalities, including rectal or uterine prolapse.
In certain cases, an arm span greater than height may be observed, though conditions like Marfan's Syndrome should be considered first when this feature is present.
The combination of the Beighton score (a scale used to assess joint hypermobility) and the EDS Diagnostic Checklist improves diagnostic accuracy. However, a detailed medical history and physical examination remain essential in identifying systemic features of EDS.

Areas Considered when Diagnosing EDS
1) A family history of the condition,
2) Recurrent musculoskeletal complications, such as limb pain lasting more than three months,
3) Widespread pain, and
4) Spontaneous joint dislocations or instability without significant trauma.
In older patients, arthritis and weight gain due to exercise intolerance may limit mobility, making the patient’s history even more crucial for diagnosis.
Many rheumatologists refer patients for evaluation of autonomic dysfunction after excluding other connective tissue diseases. Additionally, some EDS patients are mistakenly labeled with Fibromyalgia due to symptom overlap.
Other connective tissue disorders, such as Lupus, Rheumatoid Arthritis, and Scleroderma, should be ruled out, as they also affect collagen and connective tissue and may cause joint hypermobility along with other potentially life-threatening complications.
Unfortunately, there is no definitive blood test, lab test, or imaging study to confirm an EDS diagnosis; it remains a clinical diagnosis based on symptoms and history.
No standardized genetic test has been identified for EDS. Some patients present with this syndrome without a family history, despite a thorough search by their physician. These cases are rare, and the exact percentage is unknown.
While diagnosing hypermobile Ehlers-Danlos Syndrome is not necessarily difficult, it requires a thorough history and physical examination. A detailed family history is also critical, sometimes necessitating the examination of family members.
Ruling out other hereditary connective tissue disorders is essential, often requiring consultation with a skilled rheumatologist and an expert in the autonomic nervous system. Genetic testing may help exclude vascular-type EDS, Marfan’s Syndrome, and other related connective tissue diseases.
Dr. Colombo's eBook
Get your free EDS eBook!
We love to share information! Enter your information below, we will get you your copy of Dr. Colombo's EDS eBook completely free.
about the author

Dr. Joseph Colombo
Background
Dr. Colombo is trained in neurology with a background in electrical and mechanical engineering. His focus is Neuro-Cardiology. His doctorate from University of Rochester Medical School, NY, is in Neuroscience and Biomedical Engineering.
For over 25 years, Dr. Colombo has developed P&S nervous system technologies and has researched and published clinical applications and outcome studies in uses of non-invasive P&S monitoring in critical care (trauma and sepsis), anesthesiology, cardiology, endocrinology, family medicine, internal medicine, pain management, neurology, neonatology, pediatrics, psychiatry, pulmonology, sleep medicine, and more as positive, patient outcomes data are available.
He has (co-)authored over 100 journal articles internationally, and has ghost-written over 100 more. He has also (co-)authored book chapters and medical textbooks on clinical applications of, and outcomes from, non-invasive P&S guided therapy.
Dr. Colombo continues to participate in more than 50 clinical research projects world-wide and consults with physicians, clinically, on a global scale.
He has a wife of almost 40 years and two married children, and a grandchild, with over 30 years of mentoring hundreds of youths and students, including medical students.
Types of EDS
Ehlers-Danlos Syndrome (EDS) refers to a group of connective tissue disorders caused by genetic defects affecting collagen production. Here is a list of the different types of EDS and how they are characterized:
Hypermobile EDS
Characterized primarily by joint hypermobility affecting both large and small joints, which may lead to recurrent joint dislocations and partial dislocations.
Classical EDS
Associated with extremely stretchy, smooth skin that is fragile and bruises easily; wide, atrophic (flat or depressed) scars; and joint hypermobility. Molluscoid pseudotumors, calcified hematomas over pressure points such as the elbow, and spheroids, fat-containing cysts on forearms and shins, are also frequently seen. Hypotonia and delayed motor development may occur.
Dermatosparaxis EDS
Associated with extremely fragile skin leading to severe bruising and scarring; saggy, redundant skin, especially on the face; and hernias
Vascular EDS
Characterized by thin, translucent skin that is extremely fragile and bruises easily. Arteries and certain organs such as the intestines and uterus are also fragile and prone to rupture. People with this type typically have short stature; thin scalp hair; and characteristic facial features including large eyes, a thin nose, and lobeless ears. Joint hypermobility is present, but generally confined to the small joints (fingers, toes). Other common features include club foot; tendon and/or muscle rupture; acrogeria, defined as premature aging of the skin of the hands and feet; early onset varicose veins; pneumothorax, collapse of a lung; recession of the gums; and a decreased amount of fat under the skin.
Kyphoscoliosis EDS
Associated with severe hypotonia, decreased muscle tone, at birth, delayed motor development, progressive scoliosis (present from birth), and scleral fragility. Affected people may also have easy bruising; fragile arteries that are prone to rupture; unusually small corneas; and osteopenia, defined as low bone density. Other common features include a "marfanoid habitus" which is characterized by long, slender fingers (medically termed: arachnodactyly); unusually long limbs; and a sunken chest (medically termed: pectus excavatum) or protruding chest (medically termed: pectus carinatum).
Brittle Cornea Syndrome BCS
Characterized by thin cornea, early onset progressive keratoglobus, a degenerative non-inflammatory disorder of the eye in which structural changes within the cornea cause it to become extremely thin and change to a more globular shape than its normal gradual curve; and blue sclerae, described as a bluish coloration of the whites of the eyes.
Arthrochalasia EDS
Characterized by severe joint hypermobility and congenital hip dislocation. Other common features include fragile, elastic skin with easy bruising; hypotonia; kyphoscoliosis (kyphosis and scoliosis); and mild osteopenia.
Classical-like EDS
(clEDS) - Characterized by skin hyperextensibility with velvety skin texture and absence of atrophic scarring, generalized joint hypermobility (GJH) with or without recurrent dislocations (most often shoulder and ankle), and easily bruised skin or spontaneous ecchymoses (discolorations of the skin resulting from bleeding underneath).
Spondylodysplastic EDS
(spEDS) - Characterized by short stature (progressive in childhood), muscle hypotonia (ranging from severe congenital, to mild later-onset), and bowing of limbs.
Musculocontractural EDS
(mcEDS) - Characterized by congenital multiple contractures, characteristically adduction-flexion contractures and/or talipes equinovarus (clubfoot), characteristic craniofacial features, which are evident at birth or in early infancy, and skin features such as skin hyperextensibility, easy bruisability, skin fragility with atrophic scars, increased palmar wrinkling.
Myopathic EDS
(mEDS) - Characterized by congenital muscle hypotonia, and/or muscle atrophy, that improves with age, Proximal joint contractures (joints of the knee, hip and elbow); and hypermobility of distal joints (joints of the ankles, wrists, feet and hands).
Periodontal EDS
(pEDS) - Characterized by severe and intractable periodontitis of early onset (childhood or adolescence), lack of attached gingiva, pretibial plaques; and family history of a first-degree relative who meets clinical criteria.
Cardiac-Valvular EDS
(cvEDS) - Characterized by severe progressive cardiac-valvular problems (aortic valve, mitral valve), skin problems (hyperextensibility, atrophic scars, thin skin, easy bruising) and joint hypermobility (generalized or restricted to small joints).
Be a part of this life-changing mission!
Get In Touch
Assistance Hours
Monday – Friday 9:00am – 5:00pm
Saturday & Sunday – CLOSED
Email:
Phone Number:
(445) 455-4600